Nature Knows and Psionic Success
God provides
Plasma Aβ42 and Total Tau Predict Cognitive Decline in Amnestic Mild Cognitive Impairment
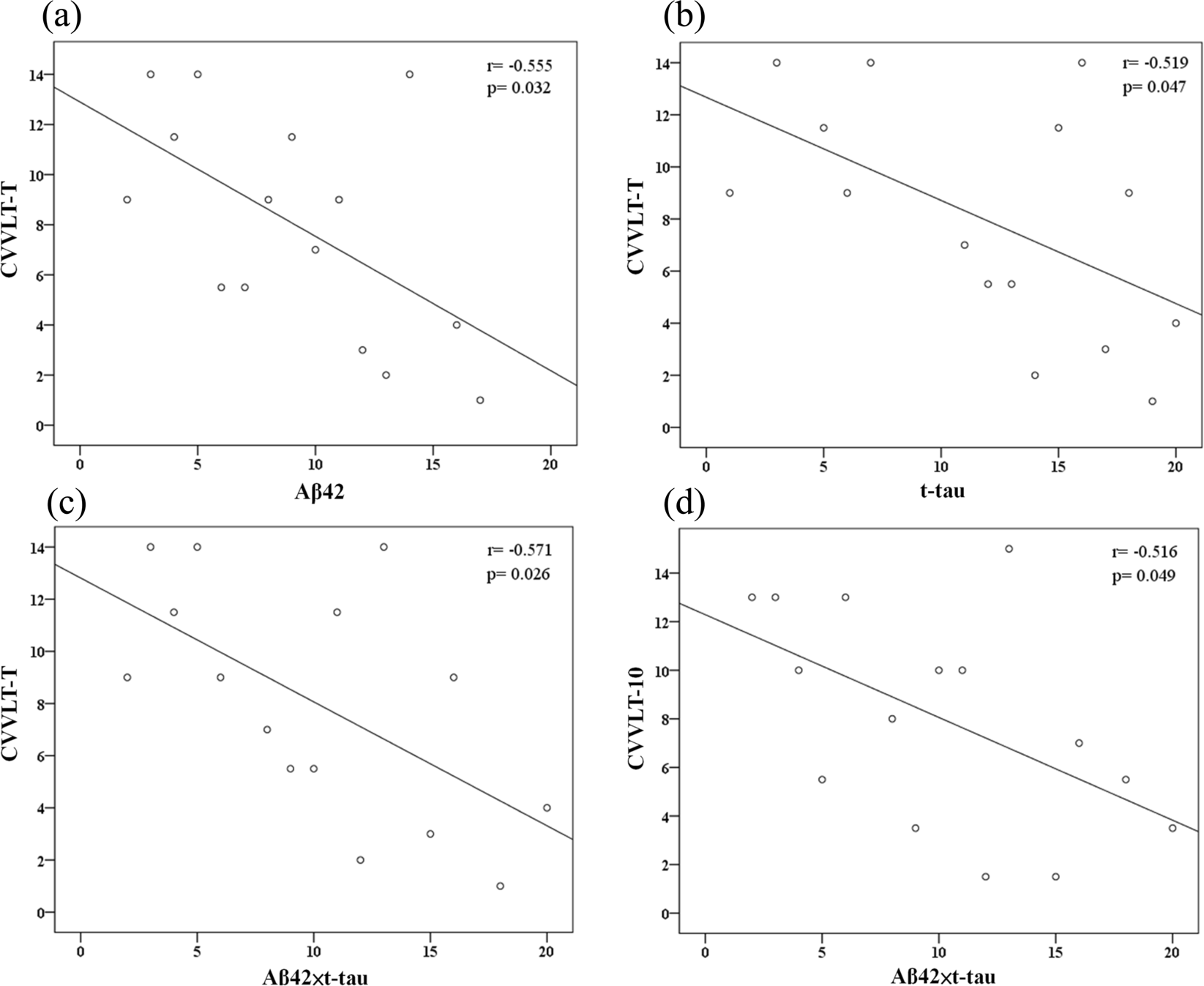
Abstract Levels of amyloid-β (Aβ) and tau peptides in brain have been associated with Alzheimer disease (AD). The current study investigated the abilities of plasma Aβ42 and total-tau (t-tau) levels in predicting cognitive decline in subjects with amnestic mild cognitive impairment (MCI). Plasma Aβ42 and t-tau levels were quantified in 22 participants with amnestic MCI through immunomagnetic reduction (IMR) assay at baseline. The cognitive performance of participants was measured through neuropsychological tests at baseline and annual follow-up (average follow-up period of 1.5 years). The predictive value of plasma Aβ42 and t-tau for cognitive status was evaluated. We found that higher levels of Aβ42 and t-tau are associated with lower episodic verbal memory performance at baseline and cognitive decline over the course of follow-up. While Aβ42 or t-tau alone had moderate-to-high discriminatory value in the identification of future cognitive decline, the product of Aβ42 and t-tau offered greater differential value. These preliminary results might suggest that high levels of plasma Aβ42 and t-tau in amnestic MCI are associated with later cognitive decline. A further replication with a larger sample over a longer time period to validate and determine their long-term predictive value is warranted. Introduction Mild cognitive impairment (MCI) refers to a transitional state on the continuum of cognitive function between normal aging and mild dementia. Amnestic MCI, characterized by an isolated deficit in episodic memory accompanied by intact general cognitive functioning, has been associated with biomarkers for Alzheimer disease (AD) and is now recognized as a risk factor for AD 1 , 2 , 3 , 4 . Early identification of subsequent cognitive decline in MCI patients is critical for prompt clinical intervention and therapeutic options. Thus, seeking validated biomarkers for risk of cognitive decline is crucial. To date, validated biomarkers associated with AD include measurement of brain Aβ […]
Click here to view full article

The Power Within by Corey Daniels book available for only $2.99
Mind has both conscious and subconscious halves. These are likened to a driver and the truck he drives. The driver plans the destination and observes road conditions, while the truck provides motive power. Your subconscious mind is like the truck and it only goes in the direction in which is a steered. This can be the road or off a cliff. Likewise, the consciousness paints a picture of what the world is and what your goals are and the subconscious acts on them through emotion, physical response and energy, whether these are correct, rational images or false negative ones. The subconscious is also like an emotional reservoir which your body and mind draw responses from to external stimuli.
The Power Within lays out a method of programming your subconscious and tapping into the Holy Spirit, God voice or what the Greeks called the daimon (godman).